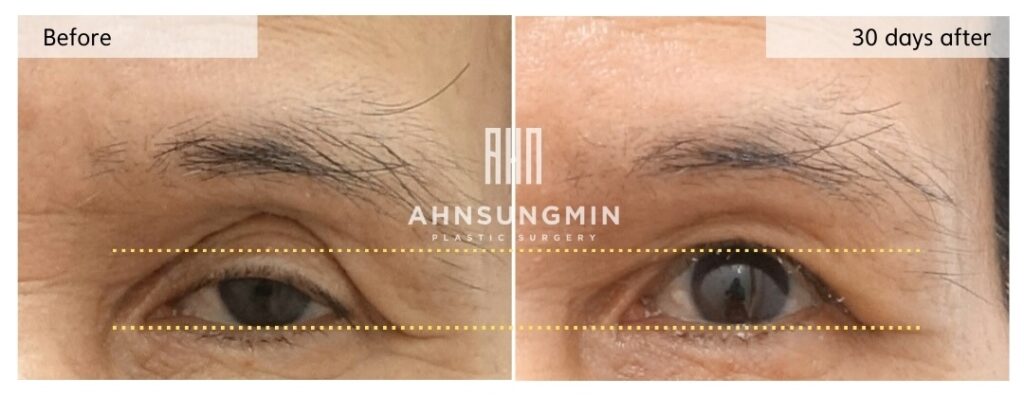
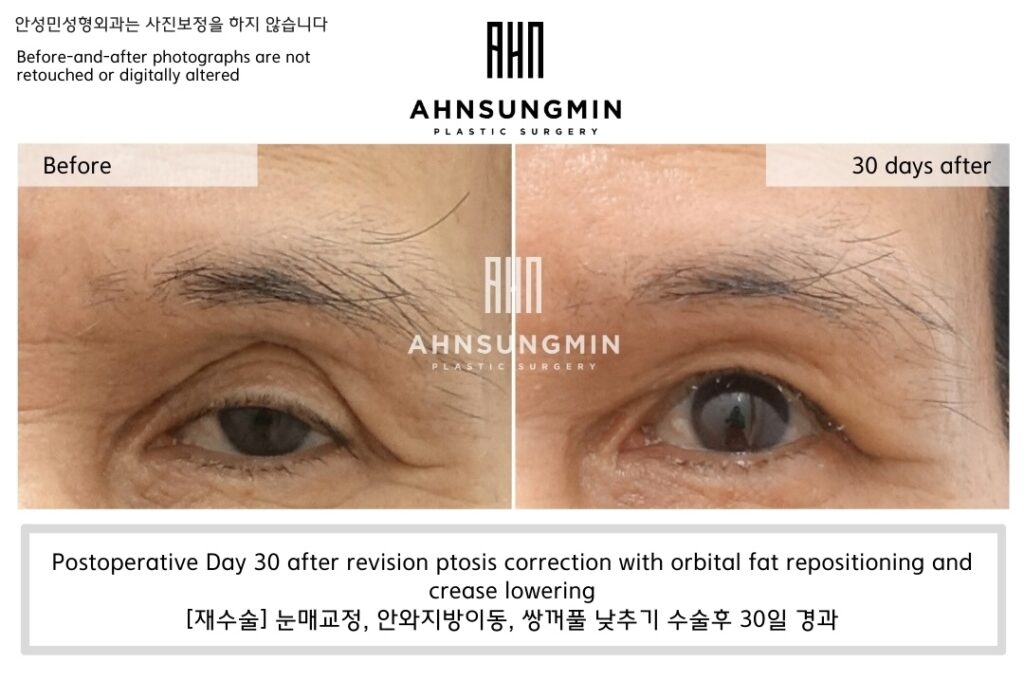
[ Before / Postoperative Day 30]
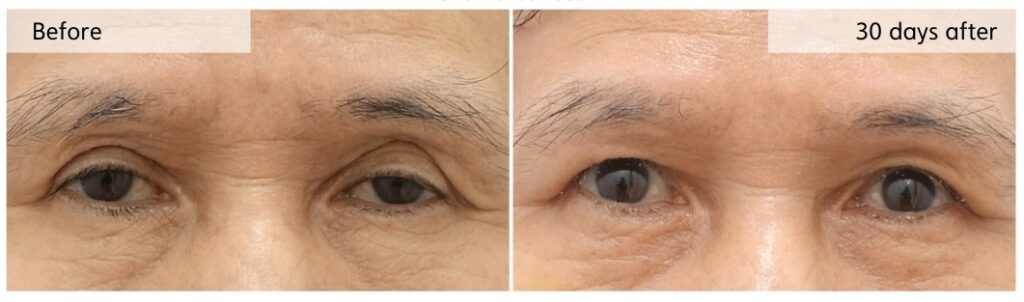
Postoperative Day 30 after revision ptosis correction with orbital fat repositioning and crease lowering
Eyelid hollowing is often approached as a problem of volume deficiency.
As a result, fat grafting is frequently suggested as the solution.
In this case, however, adding volume was not the correct answer.
The patient had already undergone fat grafting—three times.
This patient had previously received upper eyelid fat grafting three times at another clinic.
Despite repeated attempts, the hollowed appearance continued to recur.
This history alone suggested that simple volume replacement was not addressing the real problem.
The hollowing was not caused by true volume loss.
At first glance, the upper eyelid appeared sunken.
However, careful evaluation showed that orbital fat volume itself was not significantly depleted.
Instead, the eyelid had been chronically overstretched.
Compensatory eyebrow elevation and repetitive eyelid tension had altered how the tissue rested, creating the appearance of hollowing without actual volume loss.
Filling what looked hollow would not have corrected this mechanism.
Why fat grafting was not appropriate in this case.
Free fat grafting involves transferring fat that is completely disconnected from its original blood supply.
In the eyelid—where movement is constant and dynamic—fat survival is inherently unpredictable.
Even when grafted repeatedly, fat does not always survive as expected.
Irregular resorption, contour issues, and recurrence of hollowing are common.
In this patient, repeated fat grafting had already demonstrated these limitations.
For these reasons, fat grafting was not selected again.
We chose orbital fat repositioning instead.
Although the amount of remaining orbital fat was limited,
we carefully mobilized and repositioned as much of the patient’s own orbital fat as possible.
By preserving its native blood supply, orbital fat repositioning allows volume support to be restored in a more stable and physiologic way.
Rather than adding transplanted tissue, we worked within the patient’s existing anatomy.
Restoring balance, not adding volume.
In addition to orbital fat repositioning, revision ptosis correction and crease lowering were performed.
By improving eyelid function and reducing compensatory effort, excessive tension on the upper eyelid was relieved.
As eyelid movement normalized, the hollowed appearance gradually improved on its own.
No additional volume was added.
The outcome confirmed the decision.
Over time, the upper eyelid contour became smoother and more stable.
The hollowed appearance improved without introducing foreign or transplanted tissue.
This case illustrates a key principle in eyelid revision surgery.
Eyelid hollowing should not be treated based on appearance alone.
The decision is not about what can be added, but about what truly needs to be corrected.
Seeing the Eye as a Whole, Not in Parts
A Clinic Dedicated to Eyelid Revision Surgery in Korea
Ahnsungmin Plastic Surgery