
The patient’s primary concern was functional rather than cosmetic.
The eyes felt heavy and difficult to open, creating a constant sense of discomfort.
To compensate, the patient relied on forehead elevation to keep the eyes open.
The request was clear:
to see the dark pupil more clearly,
to relieve the sleepy, tired appearance,
and to lower an excessively high fold.
The patient had already undergone two previous surgeries at another clinic, both focused on lowering the fold.
The problem was not only the height of the fold.
The original crease was positioned too high and fixed very aggressively.
With repeated attempts to lower the line, scar tissue accumulated and tissue memory became dominant.
At this stage, the eyelid no longer behaved like untreated tissue.
Even after releasing the crease, the tissue continued to pull the eyelid back toward the original fixation.
As a result, part of the crease followed the previous line, and a double crease formed.
This was not an unexpected complication.
It was the predictable behavior of scar-dominant tissue after repeated fold lowering.
Our approach focused on function, not repeated correction.
Lowering the fold alone was not sufficient in this case.
We lowered the high fold and performed eyelid correction to restore comfortable eyelid opening.
By reducing the need for compensatory effort, the eyelid no longer relied on excessive force to stay open.
Once function improved, the behavior of the tissue also changed.
Residual scarring reflects limitation, not failure.
When the original crease is positioned excessively high, some degree of scarring is unavoidable.
In this patient, the previous crease had been fixed too strongly for complete erasure.
Although the high fold was lowered, traces of the previous fixation remain.
This does not represent surgical failure.
It reflects the realistic limits imposed by scar-dominant tissue.
At this stage, further manipulation would not improve the outcome.
Additional attempts to “correct” the crease would only increase instability and scarring.
For this reason, no further surgery was recommended.
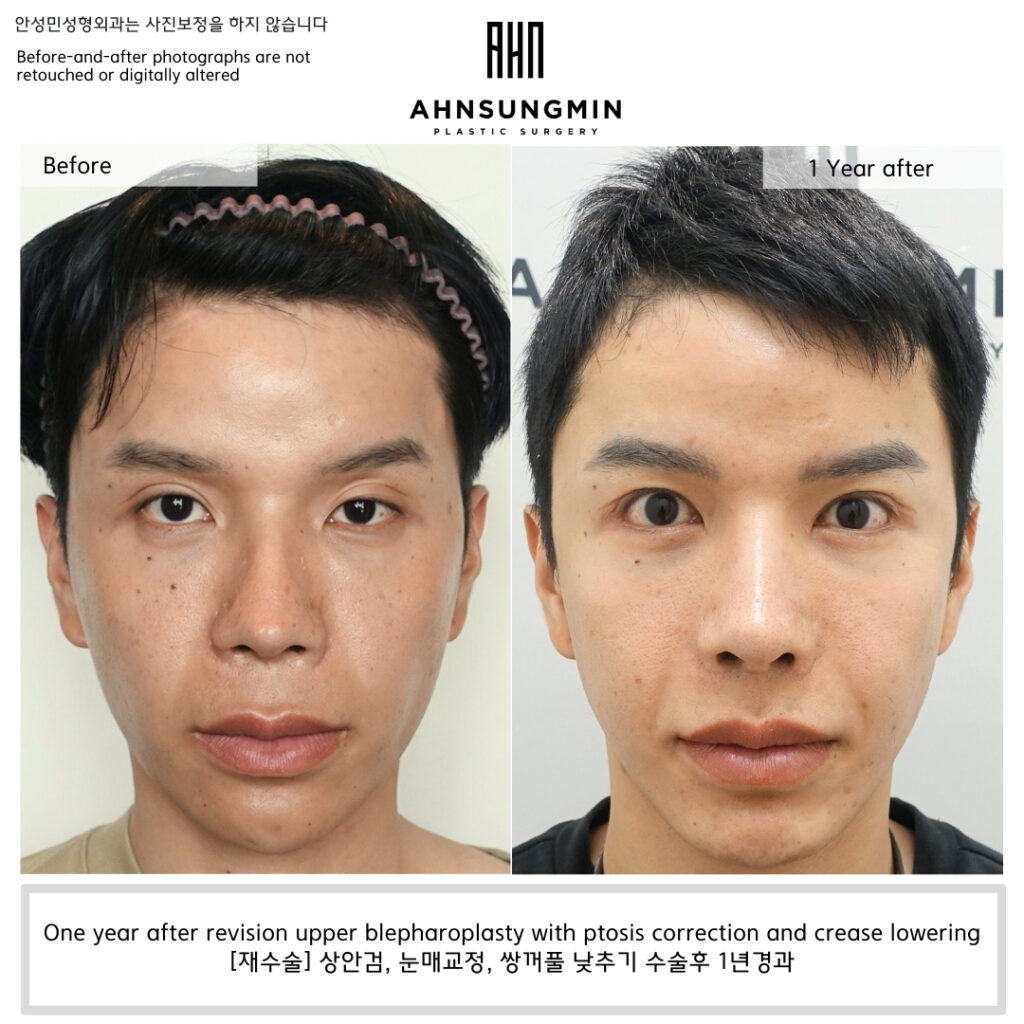
At one year after surgery, the result of ptosis correction remains stable.
Eyelid opening is well maintained without compensatory effort,
and there has been no recurrence of functional discomfort.
This long-term stability confirms that addressing function—rather than repeatedly adjusting the crease—was the correct decision in this case.
The outcome prioritized stability.
Eyelid opening is now stable and comfortable.
Functional discomfort has resolved.
The patient is very satisfied with the result.
In revision surgery, success is not defined by how much more can be changed,
but by knowing when the best result has already been achieved.
Seeing the Eye as a Whole, Not in Parts
A Clinic Dedicated to Eyelid Revision Surgery in Korea
Ahnsungmin Plastic Surgery